[ad_1]
Abstract
The International League of Dermatological Societies (ILDS), a global, not-for-profit organization representing 157 dermatological societies worldwide, has identified the consequences of skin aging as one of the most important grand challenges in global skin health. Reduced functional capacity and increased susceptibility of the skin with development of dermatoses such as dry skin, itching, ulcers, dyspigmentation, wrinkles, fungal infections, as well as benign and malignant tumors are the most common skin conditions in aged populations worldwide. Environmental (e.g., pollution) and lifestyle factors (e.g., smoking, sunbed use) negatively affect skin health. In turn altered appearance, dry skin, chronic wounds, and other conditions decrease general health and reduce the likelihood for healthy and active aging. Preventive skin care includes primary, secondary, and tertiary interventions. Continuous sun protection from early childhood onward is most important, to avoid extrinsic skin damage and skin cancer. Exposure to irritants, allergens, or other molecules damaging the skin must be avoided or reduced to a minimum. Public health approaches are needed to implement preventive and basic skin care worldwide to reach high numbers of dermatological patients and care receivers. Education of primary caregivers and implementation of community dermatology are successful strategies in resource-poor countries. Besides specialist physicians, nurses and other health care professionals play important roles in preventing and managing age-related skin conditions in developing as well as in developed countries. Healthy skin across the life course leads to better mental and emotional health, positive impact on social engagement, and healthier, more active, and productive lives.
The skin is the largest organ of the human body that fulfills multiple essential tasks. It forms the boundary between the inside and outside. It provides protection against mechanical and chemical threats, it provides innate and adaptive immune defenses, it enables thermoregulation and vitamin D production, and it acts as the sensory organ of touch ( Chuong et al., 2002 ). Like every other complex biological system, the skin grows, matures, and ages throughout the life course. Skin aging is associated with a reduction in functional capacity that itself increases the susceptibility to cutaneous problems and the subsequent development of dermatoses and skin cancers. As well as changes in cutaneous structure and function, its appearance is the key observable marker of the overall aging process. Thus, our physical appearance in advanced age is important for emotional, mental, and psychosocial well-being ( Gupta, 2010 ).
The International League of Dermatological Societies (ILDS) is a global, not-for-profit organization that represents 157 dermatological societies and 150,000 dermatologists worldwide. The ILDS, at a meeting in London in November 2013, identified and prioritized skin aging and its consequences as one of the most important grand challenges in global skin health. The objective of this contribution is to provide background information about the mechanisms of skin aging and the resulting clinical implications. Epidemiological figures about the most prevalent age-associated skin conditions are summarized to indicate the burden of cutaneous conditions in the elderly worldwide. We describe the main gaps and challenges associated with skin aging and argue why a public health approach is needed. Finally, based on the findings of this background paper and on Consensus Statements of an ILDS led summit “A Life Course of Active Ageing and Healthy Skin” ( Global Coalition on Aging, 2014 ) held in Manchester (United Kingdom) in June 2014, recommendations from a public health and skin health promotion point of view will be given.
Mechanisms of Skin Aging
Intrinsic and Extrinsic Skin Aging
Natural aging is a time-dependent phenomenon that results in specific changes to the appearance and function of human skin. However, we also interact with our environment. Hence, “aging” must be seen as the composite of two biological processes: natural—or intrinsic—aging and those changes brought about by our skin’s interaction with the external environment—termed extrinsic aging. Lifestyle choices greatly affect the appearance and function of skin, and there is significant evidence that the major environmental factor that influences skin biology is chronic sun exposure (ultra violet radiation [UVR]). There is also increasing evidence that smoking ( Daniell, 1971 ; Kadunce et al., 1991 ; Martires, Fu, Polster, Cooper, & Baron, 2009 ), hormonal status ( Bolognia, Braverman, Rousseau, & Sarrel, 1989 ; Brincat et al., 1983 ; Emmerson & Hardman, 2012 ), and environmental pollution ( Krutmann et al., 2014 ) contribute to the appearance of aged skin. As both intrinsic and extrinsic aging result in a common endpoint—the decline of skin’s physiological function—it is tempting to think of extrinsic aging as an acceleration of those processes that occur in intrinsic aging. Clinically, signs of intrinsically aged skin rarely manifest before the age of 70 years; skin is pale and dry and is characterized by fine wrinkles alone. However, in areas that have been exposed to chronic solar UVR, the clinical appearance is strikingly different; skin appears sallow and roughened and often presents with hypo- and hyperpigmented lesions (age spots). Extrinsically aged skin also features coarse wrinkles with increased laxity, especially in areas of dynamic change due to facial expression such as periorbital “crow’s feet.” Yet, it must be emphasized that although these external environmental factors can accelerate and more deeply affect skin deterioration as we age, there are none of us who will escape the effects to some degree.
Pathophysiology of Aged Skin
Skin is composed of two major, and functionally distinct, layers. The outermost epidermis is highly cellular and avascular, consisting predominantly of keratinocytes. It provides a physical barrier between the individual and the external environment, preventing water loss, providing protection from infection (both as a physical barrier and via immune cells; Fuchs, 2009 ). The dermis, by comparison, is relatively cell-poor and is composed largely of a complex extracellular matrix (ECM) that provides skin with strength, resilience, and compliance. It supports the organ by housing complex vascular, lymphatic, and neuronal systems. Between these two distinct layers is the dermal-epidermal junction (DEJ), a complex basement membrane zone critical for intercellular communication and cohesion. All skin layers show age-related alterations in terms of their structure and function. The aged epidermis is atrophic ( Lavker, Zheng, & Dong, 1987 ) with diminution of rete pegs and ridges ( Giangreco, Goldie, Failla, Saintigny, & Watt, 2010 ; Hull & Warfel, 1983 ). Functionally, the aged epidermis shows a reduced capacity for barrier function and repair following insult ( Choi et al., 2007 ). Lipid processing declines with advancing age; enzymes necessary for the production of ceramides critical to healthy epidermal barrier function are all diminished in the elderly ( Jensen et al., 2005 ). Epidermal CD44, the keratinocyte transmembrane glycoprotein thought to play a regulatory role in keratinocyte proliferation and maintaining local hyaluronic acid homeostasis, decreases with increasing age ( Kaya & Saurat, 2007 ; Kaya et al., 2006 ) and may contribute to epidermal thinning and reduction in its viscoelastic properties. Such epidermal alterations increase the susceptibility to a wide range of skin problems: colonization by pathogenic bacteria; reduced stratum corneum cohesion and hydration, leading to dry skin and pruritus, conditions highly prevalent in aged individuals leading to a substantial negative impact on quality of life ( Chang, Wong, Endo, & Norman, 2013 ; Garibyan, Chiou, & Elmariah, 2013 ). Flattening of the DEJ may contribute to skin fragility that is often observed clinically with increasing age. Alterations in the expression of component molecules are thought to contribute to reduced cohesion in aged individuals ( Hatje, Richter, Blume-Peytavi, & Kottner, 2015 ) predisposing to shear-type injuries and bulla formation ( Gilchrest, 1986 ).
The dermal ECM exhibits structural and functional changes in both intrinsically and extrinsically aged skin. The dermis of a young individual is a complex association of fibrillar collagens, microfibrillar proteins, and elastic fibers embedded in a proteoglycan-rich ground substance. These diverse ECM molecules confer different characteristics to the skin; collagen is thought to provide tensile strength, elastin contributes to resilience and capacity for recoil, whereas proteoglycans are important for hydration. Such molecules are long-lived, as compared with their intercellular counterparts ( Ritz-Timme, Laumeier, & Collins, 2003 ; Shapiro, Endicott, Province, Pierce, & Campbell, 1991 ) and so any tissue rich in these long-lived ECM assemblies has the potential to accrue damage in the long term. Accumulated damage results in structural and, consequently, functional sequelae to the dermal ECM ( Bailey, 2001 ) that may underlie the clinical features of intrinsically and extrinsically aged skin ( Warren et al., 1991 ). The major fibrillar collagens found within the dermis are type I and type III; they are the most abundant by dry weight and form extended arrays of fibrils thought to confer tensile strength ( Daly, 1982 ). These large assemblies are laid down in an interwoven “basket weave” arrangement ( Graham et al., 2010 ) that is in stark contrast to tissues such as tendon and cornea where collagen fibrils have distinct directionality ( Karamichos, Lakshman, & Petroll, 2007 ; Whittaker & Canham, 1991 ). With increasing age, atrophy of the dermal matrix occurs including a reduction in the deposition of type I and type III collagens ( Lovell et al., 1987 ; Pearce & Grimmer, 1972 ). Synthesis of these ECM molecules is also impaired ( Autio, Risteli, Haukipuro, Risteli, & Oikarinen, 1994 ; Furth, 1991 ). Elastic fibers are insoluble structural elements of connective tissues that have a central core of amorphous, hydrophobic cross-linked elastin surrounded by fibrillin-rich microfibrils that confer compliance and recoil to the skin; their formation is under tight developmental control. Disintegration of elastic fibers are observed in intrinsically aged skin ( Braverman & Fonferko, 1982 ) and this correlates with a loss of fibulin-5-positive elastic fibers in intrinsic aging ( Kadoya et al., 2005 ); this atrophy is in contrast with the appearance of the elastic fiber in skin exposed to UV, where solar elastosis—the deposition of disorganized, dystrophic material—is the key histological finding ( Dawber & Shuster, 1971 ). The collagenous and elastic matrices are embedded in a carbohydrate-rich “ground substance”; these hydrophilic molecules, in conjunction with hyaluronic acid ( Reed, Lilja, & Laurent, 1988 ), are distributed throughout the dermis where they perform a key role in maintaining skin hydration.
Functional Capacity and Aging Skin
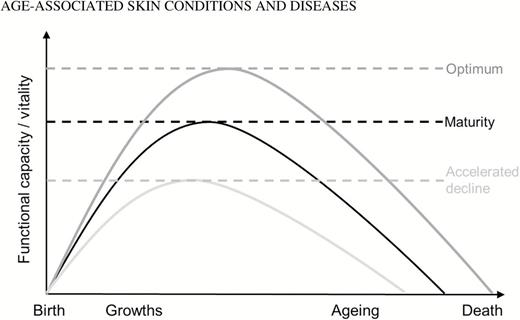
Numerous models have been proposed to describe and to measure the natural course of human aging ( Beier, 1985 ; Kuh, Richards, Cooper, Hardy, & Ben-Shlomo, 2014 ). The concept of the functional capacity (or vitality) over the life course ( Ruiz-Torres, Agudo, Vicent, & Beier, 1990 ) is a useful theoretical framework to connect the chronological aging process with functional and psychosocial parameters. Functional capacity is the ability of complex biological systems to cope with external stress. Accordingly, interventions creating supportive environments and healthy living are able to increase the functional capacity enabling longer and healthier lives ( World Health Organization, 2002 ). On the contrary, the repeated exposure to and the accumulation of detrimental insults during the life span accelerate functional decline leading to (early) illness, disability, impairments, and death (see Figure 1 ). These life course functional trajectories can be applied to human aging in general and to distinct organ systems ( Kuh et al., 2014 ). Hence, this model is applicable to the skin.
Figure 1.

Functional capacity over the life course.
For instance, as described above, lifelong and repeated exposure to UVR damages the skin leading to benign and to malignant skin changes. Indeed, the incidence of skin cancers and associated morbidity and mortality is increasing worldwide and explicitly with age. Skin cancers are the most frequent cancers overall ( Boyers et al., 2014 ; Jurciukonyte, Vincerzevskiene, Krilaviciute, Bylaite, & Smailyte, 2013 ; Mayer, Swetter, Fu, & Geller, 2014 ). At the same time, there is substantial evidence that minimizing UV exposure via sun-smart lifestyle choices and early detection and treatment of cutaneous lesions such as preclinical skin cancers are key to maintaining a healthy skin ( Al-Nuaimi, Sherratt, & Griffiths, 2014 ; Elsner et al., 2007 ). Thus, there is a huge potential to prevent skin cancers by implementing healthy living styles ( Ryan, 1998 ).
Another modifiable lifestyle factor directly damaging skin structure and function in the long term is smoking. On one hand, smoking accelerates signs of skin aging enhancing the unwanted appearance of “looking old” ( Dobos, Lichterfeld, Blume-Peytavi, & Kottner, 2015 ). On the other hand, smoking decreases the cutaneous strength, impairs wound healing and connective tissue turnover, and slows epidermal regeneration ( Sherwin & Gastwirth, 1990 ; Sørensen et al., 2010 ).
The two aforementioned examples clearly indicate how external factors negatively affect the skin function during the life course. In addition, there is convincing evidence that accumulating skin aging–related problems are major factors of functional decline in general.
Chronic Wounds
Advanced age and activity and mobility impairments with or without cardiovascular diseases and diabetes mellitus, which are most frequent in older people, are strong predictors for developing chronic wounds like venous, pressure, or diabetic foot ulcers ( Gould et al., 2015 ; Hay et al., 2014 ; Morrone, 2008 ). The presence of such wounds causes pain and further diminishes mobility and social activity ( Morrone, 2008 ). Ulcers cause negative emotional impacts including feelings of fear, social isolation, anger, depression, and negative self-image, which further contributes to overall health deterioration ( Gorecki et al., 2009 ; Sen et al., 2009 ).
“Looking Old”
The pure fact of “looking old” or “ugly” has substantial negative effects on self-esteem, social interactions and thus it has enormous social and cultural relevance ( Gupta & Gilchrest, 2005 ; Ryan, 1992 ). The perceptions of an aged appearance are influenced by ethnic and cultural factors that vary widely across the globe. However, there seems to be no place today where a wrinkled and mottled appearance enhances social appreciation and acceptance. For instance, pigmentary anomalies especially in darker-skinned individuals are a great source of psychological concern based on strong sociological roots ( Verma, 2011 ). In Western societies, youthfulness is considered a key component of attractiveness ( Farage, Miller, Berardesca, & Maibach, 2010 ; Gupta & Gilchrest, 2005 ). Having no confidence in one’s appearance prohibits active and successful participation and failure to achieve one’s potential ( Morrone, 2008 ). At the worst, an aged appearance contributes to “ageism” that is still very common in medicine and health care ( Aronson, 2015 ).
Dry Skin
Dry skin (xerosis cutis) is one of the most prevalent conditions in the aged worldwide ( Al-Nuaimi et al., 2014 ). Severe forms of dry skin lead to sleep deprivation; pruritus and constant scratching cause even more severe forms including cracks, bleeding, and infection decreasing the overall quality of life substantially ( Berger, Shive, & Harper, 2013 ; White-Chu & Reddy, 2011 ).
Skin Health Promotes Healthy Aging
The selected examples above indicate that aging increases the likelihood of developing a variety of age-associated skin conditions. In turn, these chronic skin conditions have a direct effect on overall functional and psychosocial capacity, well-being, and health (see Figure 2 ). Thus, improving skin health directly promotes healthy and active aging.
Figure 2.

Skin aging affects functional capacity and social participation.
Epidemiology of Aging-Related Skin Conditions and Diseases
Comprehensive epidemiological figures about the frequencies of age-related skin conditions are rare, which underscores the profound and driving need for greater attention to a life course approach of healthy skin in an era of longevity. Using the search strategy of comprehensive systematic review about the epidemiology of skin conditions in the aged, we identified primary studies reporting prevalence and/or incidence in people aged at least 65 years and older. For this contribution, in addition to the inclusion criteria outlined in the full review protocol ( Hahnel, Lichterfeld, Blume-Peytavi, & Kottner, 2014 ), the inclusion period was extended before 2000. Based on the reported findings, skin conditions were classified according to the recent WHO ICD-10 version 2015 ( World Health Organization, 2015 ).
In total, five studies were identified for institutional long-term care settings in Europe, Northern America, and Asia (see Table 1 ). Xerosis was the most prevalent skin problem in this setting (up to 85%) followed by fungal diseases (up to 57%). Nonmalignant skin changes including lentigines and seborrheic keratoses were so common (up to 87%) that nearly every recipient of long-term care included in these studies was affected.
Frequencies of Skin Conditions in Long-Term Care
| Country | Denmark (Weismann, Krakauer, & Wanscher, 1980) | United States (Beauregard & Gilchrest, 1987) | United States (Fleischer, McFarlane, Hinds, & Mittelmark, 1996) | Taiwan (Smith et al., 2002) | Turkey (Kiliç, Gül, Aslan, & Soylu, 2008) |
|---|---|---|---|---|---|
| Setting | Nursing home | Home care | Home care | Nursing home | Nursing home |
| Year | 1980 | 1987 | 1996 | 2002 | 2008 |
| n | 584 | 68 | 204 | 398 | 300 |
| Age (years) | 80.0 ( SD no data) | 74.0 ( SD no data) | 75.0 ( SD 4.6) | 76.2 ( SD 9.9) | 76.4 ( SD 7.8) |
| Type of estimate | Prevalence (%) | Prevalence (%) | Prevalence (%) | Prevalence (%) | Prevalence (%) |
| B35.1 Tinea unguium (incl. onychomycosis) | No data | No data | 51.0 | 57.3 | 34.7 |
| B35.3 Tinea pedis | No data | 17.7 | 22.1 | 34.4 | 33.0 |
| B37.2 Candidiasis of skin and nail (incl. candida intertrigo) | No data | No data | No data | No data | 3.0 |
| C43-C44 Melanoma and other malignant neoplasms of skin | No data | 4.4 | 10.8 | 0.3 | No data |
| D18 Hemangioma, any site (incl. cherry angioma) | No data | 53.7 | 85.3 | No data | No data |
| D69.2 Other nonthrombocytopenic purpura (incl. senile purpura) | No data | 11.9 | 14.7 | 1.5 | No data |
| H02.6 Xanthelasma of eyelid | 4.6 | No data | No data | No data | No data |
| I78.1 Naevus, nonneoplastic (incl. senile angioma) | No data | No data | No data | No data | 20.3 |
| I83.1 Varicose veins of lower extremities (incl. stasis dermatitis and ulcers) | 8.4 | 5.9 | 2.5 | No data | 4.3 |
| L21 Seborrheic dermatitis | 7.0 | 10.5 | 28.9 | No data | No data |
| L21.0 Seborrhoea capitis | 44.3 | 11.9 | No data | No data | No data |
| L24 Irritant contact dermatitis | 3.8 | 11.8 | 6.8 | No data | No data |
| L29 Pruritus | No data | 29 | 70.0 | No data | 10.3 |
| L40 Psoriasis | 2.9 | 2.9 | No data | No data | No data |
| L57.0 Actinic keratosis | No data | 17.7 | 32.4 | No data | 29.3 |
| L57.4 Cutis laxa senilis (incl. elastosis) | No data | 95.6 | No data | No data | No data |
| L60 Nail disorders (incl. onychorrhexis, onychauxis) | No data | 85.1 | 19.6 | No data | No data |
| L70/71 Acne/rosacea | 0.2 | 7.4 | 8.8 | No data | No data |
| L80 Vitiligo | 1.2 | No data | No data | No data | No data |
| L81.4 Other melanin hyperpigmentation (incl. lentigines) | No data | 70.6 | 86.8 | No data | No data |
| L82 Seborrheic keratosis (incl. dermatosis papulosa nigra) | No data | 61.2 | 85.3 | No data | 11.3 |
| L85.3 Xerosis cutis (incl. eczema craqueleé) | 28.9 | 85.1 | 60.3 | 58.3 | 45.3 |
| L89 Pressure ulcer | 2.2 | No data | No data | 1.8 | No data |
| L92.0 Granuloma annulare | No data | 2.9 | No data | No data | No data |
| Country | Denmark (Weismann, Krakauer, & Wanscher, 1980) | United States (Beauregard & Gilchrest, 1987) | United States (Fleischer, McFarlane, Hinds, & Mittelmark, 1996) | Taiwan (Smith et al., 2002) | Turkey (Kiliç, Gül, Aslan, & Soylu, 2008) |
|---|---|---|---|---|---|
| Setting | Nursing home | Home care | Home care | Nursing home | Nursing home |
| Year | 1980 | 1987 | 1996 | 2002 | 2008 |
| n | 584 | 68 | 204 | 398 | 300 |
| Age (years) | 80.0 ( SD no data) | 74.0 ( SD no data) | 75.0 ( SD 4.6) | 76.2 ( SD 9.9) | 76.4 ( SD 7.8) |
| Type of estimate | Prevalence (%) | Prevalence (%) | Prevalence (%) | Prevalence (%) | Prevalence (%) |
| B35.1 Tinea unguium (incl. onychomycosis) | No data | No data | 51.0 | 57.3 | 34.7 |
| B35.3 Tinea pedis | No data | 17.7 | 22.1 | 34.4 | 33.0 |
| B37.2 Candidiasis of skin and nail (incl. candida intertrigo) | No data | No data | No data | No data | 3.0 |
| C43-C44 Melanoma and other malignant neoplasms of skin | No data | 4.4 | 10.8 | 0.3 | No data |
| D18 Hemangioma, any site (incl. cherry angioma) | No data | 53.7 | 85.3 | No data | No data |
| D69.2 Other nonthrombocytopenic purpura (incl. senile purpura) | No data | 11.9 | 14.7 | 1.5 | No data |
| H02.6 Xanthelasma of eyelid | 4.6 | No data | No data | No data | No data |
| I78.1 Naevus, nonneoplastic (incl. senile angioma) | No data | No data | No data | No data | 20.3 |
| I83.1 Varicose veins of lower extremities (incl. stasis dermatitis and ulcers) | 8.4 | 5.9 | 2.5 | No data | 4.3 |
| L21 Seborrheic dermatitis | 7.0 | 10.5 | 28.9 | No data | No data |
| L21.0 Seborrhoea capitis | 44.3 | 11.9 | No data | No data | No data |
| L24 Irritant contact dermatitis | 3.8 | 11.8 | 6.8 | No data | No data |
| L29 Pruritus | No data | 29 | 70.0 | No data | 10.3 |
| L40 Psoriasis | 2.9 | 2.9 | No data | No data | No data |
| L57.0 Actinic keratosis | No data | 17.7 | 32.4 | No data | 29.3 |
| L57.4 Cutis laxa senilis (incl. elastosis) | No data | 95.6 | No data | No data | No data |
| L60 Nail disorders (incl. onychorrhexis, onychauxis) | No data | 85.1 | 19.6 | No data | No data |
| L70/71 Acne/rosacea | 0.2 | 7.4 | 8.8 | No data | No data |
| L80 Vitiligo | 1.2 | No data | No data | No data | No data |
| L81.4 Other melanin hyperpigmentation (incl. lentigines) | No data | 70.6 | 86.8 | No data | No data |
| L82 Seborrheic keratosis (incl. dermatosis papulosa nigra) | No data | 61.2 | 85.3 | No data | 11.3 |
| L85.3 Xerosis cutis (incl. eczema craqueleé) | 28.9 | 85.1 | 60.3 | 58.3 | 45.3 |
| L89 Pressure ulcer | 2.2 | No data | No data | 1.8 | No data |
| L92.0 Granuloma annulare | No data | 2.9 | No data | No data | No data |
Frequencies of Skin Conditions in Long-Term Care
| Country | Denmark (Weismann, Krakauer, & Wanscher, 1980) | United States (Beauregard & Gilchrest, 1987) | United States (Fleischer, McFarlane, Hinds, & Mittelmark, 1996) | Taiwan (Smith et al., 2002) | Turkey (Kiliç, Gül, Aslan, & Soylu, 2008) |
|---|---|---|---|---|---|
| Setting | Nursing home | Home care | Home care | Nursing home | Nursing home |
| Year | 1980 | 1987 | 1996 | 2002 | 2008 |
| n | 584 | 68 | 204 | 398 | 300 |
| Age (years) | 80.0 ( SD no data) | 74.0 ( SD no data) | 75.0 ( SD 4.6) | 76.2 ( SD 9.9) | 76.4 ( SD 7.8) |
| Type of estimate | Prevalence (%) | Prevalence (%) | Prevalence (%) | Prevalence (%) | Prevalence (%) |
| B35.1 Tinea unguium (incl. onychomycosis) | No data | No data | 51.0 | 57.3 | 34.7 |
| B35.3 Tinea pedis | No data | 17.7 | 22.1 | 34.4 | 33.0 |
| B37.2 Candidiasis of skin and nail (incl. candida intertrigo) | No data | No data | No data | No data | 3.0 |
| C43-C44 Melanoma and other malignant neoplasms of skin | No data | 4.4 | 10.8 | 0.3 | No data |
| D18 Hemangioma, any site (incl. cherry angioma) | No data | 53.7 | 85.3 | No data | No data |
| D69.2 Other nonthrombocytopenic purpura (incl. senile purpura) | No data | 11.9 | 14.7 | 1.5 | No data |
| H02.6 Xanthelasma of eyelid | 4.6 | No data | No data | No data | No data |
| I78.1 Naevus, nonneoplastic (incl. senile angioma) | No data | No data | No data | No data | 20.3 |
| I83.1 Varicose veins of lower extremities (incl. stasis dermatitis and ulcers) | 8.4 | 5.9 | 2.5 | No data | 4.3 |
| L21 Seborrheic dermatitis | 7.0 | 10.5 | 28.9 | No data | No data |
| L21.0 Seborrhoea capitis | 44.3 | 11.9 | No data | No data | No data |
| L24 Irritant contact dermatitis | 3.8 | 11.8 | 6.8 | No data | No data |
| L29 Pruritus | No data | 29 | 70.0 | No data | 10.3 |
| L40 Psoriasis | 2.9 | 2.9 | No data | No data | No data |
| L57.0 Actinic keratosis | No data | 17.7 | 32.4 | No data | 29.3 |
| L57.4 Cutis laxa senilis (incl. elastosis) | No data | 95.6 | No data | No data | No data |
| L60 Nail disorders (incl. onychorrhexis, onychauxis) | No data | 85.1 | 19.6 | No data | No data |
| L70/71 Acne/rosacea | 0.2 | 7.4 | 8.8 | No data | No data |
| L80 Vitiligo | 1.2 | No data | No data | No data | No data |
| L81.4 Other melanin hyperpigmentation (incl. lentigines) | No data | 70.6 | 86.8 | No data | No data |
| L82 Seborrheic keratosis (incl. dermatosis papulosa nigra) | No data | 61.2 | 85.3 | No data | 11.3 |
| L85.3 Xerosis cutis (incl. eczema craqueleé) | 28.9 | 85.1 | 60.3 | 58.3 | 45.3 |
| L89 Pressure ulcer | 2.2 | No data | No data | 1.8 | No data |
| L92.0 Granuloma annulare | No data | 2.9 | No data | No data | No data |
| Country | Denmark (Weismann, Krakauer, & Wanscher, 1980) | United States (Beauregard & Gilchrest, 1987) | United States (Fleischer, McFarlane, Hinds, & Mittelmark, 1996) | Taiwan (Smith et al., 2002) | Turkey (Kiliç, Gül, Aslan, & Soylu, 2008) |
|---|---|---|---|---|---|
| Setting | Nursing home | Home care | Home care | Nursing home | Nursing home |
| Year | 1980 | 1987 | 1996 | 2002 | 2008 |
| n | 584 | 68 | 204 | 398 | 300 |
| Age (years) | 80.0 ( SD no data) | 74.0 ( SD no data) | 75.0 ( SD 4.6) | 76.2 ( SD 9.9) | 76.4 ( SD 7.8) |
| Type of estimate | Prevalence (%) | Prevalence (%) | Prevalence (%) | Prevalence (%) | Prevalence (%) |
| B35.1 Tinea unguium (incl. onychomycosis) | No data | No data | 51.0 | 57.3 | 34.7 |
| B35.3 Tinea pedis | No data | 17.7 | 22.1 | 34.4 | 33.0 |
| B37.2 Candidiasis of skin and nail (incl. candida intertrigo) | No data | No data | No data | No data | 3.0 |
| C43-C44 Melanoma and other malignant neoplasms of skin | No data | 4.4 | 10.8 | 0.3 | No data |
| D18 Hemangioma, any site (incl. cherry angioma) | No data | 53.7 | 85.3 | No data | No data |
| D69.2 Other nonthrombocytopenic purpura (incl. senile purpura) | No data | 11.9 | 14.7 | 1.5 | No data |
| H02.6 Xanthelasma of eyelid | 4.6 | No data | No data | No data | No data |
| I78.1 Naevus, nonneoplastic (incl. senile angioma) | No data | No data | No data | No data | 20.3 |
| I83.1 Varicose veins of lower extremities (incl. stasis dermatitis and ulcers) | 8.4 | 5.9 | 2.5 | No data | 4.3 |
| L21 Seborrheic dermatitis | 7.0 | 10.5 | 28.9 | No data | No data |
| L21.0 Seborrhoea capitis | 44.3 | 11.9 | No data | No data | No data |
| L24 Irritant contact dermatitis | 3.8 | 11.8 | 6.8 | No data | No data |
| L29 Pruritus | No data | 29 | 70.0 | No data | 10.3 |
| L40 Psoriasis | 2.9 | 2.9 | No data | No data | No data |
| L57.0 Actinic keratosis | No data | 17.7 | 32.4 | No data | 29.3 |
| L57.4 Cutis laxa senilis (incl. elastosis) | No data | 95.6 | No data | No data | No data |
| L60 Nail disorders (incl. onychorrhexis, onychauxis) | No data | 85.1 | 19.6 | No data | No data |
| L70/71 Acne/rosacea | 0.2 | 7.4 | 8.8 | No data | No data |
| L80 Vitiligo | 1.2 | No data | No data | No data | No data |
| L81.4 Other melanin hyperpigmentation (incl. lentigines) | No data | 70.6 | 86.8 | No data | No data |
| L82 Seborrheic keratosis (incl. dermatosis papulosa nigra) | No data | 61.2 | 85.3 | No data | 11.3 |
| L85.3 Xerosis cutis (incl. eczema craqueleé) | 28.9 | 85.1 | 60.3 | 58.3 | 45.3 |
| L89 Pressure ulcer | 2.2 | No data | No data | 1.8 | No data |
| L92.0 Granuloma annulare | No data | 2.9 | No data | No data | No data |
Eleven studies have been identified for acute inpatient and outpatient care settings in North America, Europe, and Asia (see Supplementary Table ). Seborrheic keratoses and pigmentary changes were most common (up to 93%) followed by fungal infections (up to 79%). The prevalence of malignant neoplasms of the skin ranged from 2.1% in Taiwan to 15.5% in Iran.
Disregarding methodological limitations and the proportions of missing data, some general conclusions can be drawn. The number and prevalence of dermatological conditions in older, senior populations are high. This finding is supported by the latest Global Burden of Disease Study (2010), where the years lost due to disability caused by skin conditions were highest in the aged ( Hay et al., 2014 ).
For example, according to the review, dry skin, fungal infections, and several forms of dermatitis are most prevalent across all countries and health care settings. Although clearly not life-threatening, these conditions increase the risk for more severe subsequent skin problems (e.g., cellulitis, wounds). The identified conditions usually respond well to simple treatments (e.g., emollient use to treat dry skin). Undersupply and malpractice regarding basic skin care in the elderly is highly likely, which is supported by recent epidemiological findings ( Kottner, Boronat, Blume-Peytavi, Lahmann, & Suhr, 2015 ) and expert opinion ( Cowdell, 2011 ; Cowdell & Steventon, 2015 ).
Review results also indicate high prevalences of elastosis, dyspigmentation, seborrheic keratoses, and other nonmalignant skin conditions. While cosmetically disturbing, it is important to consider that these skin conditions associated with aging (also including sagging, wrinkles) are not pathological per se. Indeed, the line between the physiological and “truly” pathological is not always clear with advancing age ( Grover & Narasimhalu, 2009 ; Tindall, 1976 ) and cosmetic procedures are considered life enhancing, rather than life saving ( Gupta, 2010 ). This does not mean that cosmetic approaches should be discounted, quite the opposite: they should be accepted as a means that may allow individuals to cope better with the aging process ( Farage et al., 2010 ), making the elderly more attractive ( Ryan, 1992 ) with positive impacts on mental and emotional health. This in turn could lead to a healthier and more active aging, which will have positive fiscal impact as well as better health outcomes for the individuals and their families ( Gupta & Gilchrest, 2005 ; Ryan, 1992 ).
Review results further indicate that epidemiological data about skin conditions in the elderly especially from developing countries are largely unavailable ( Figueroa, Fuller, Abraha, & Hay, 1998 ). This might contribute to the underestimation of age-related skin problems in general. In 2013, the top four countries with the largest populations of people being 80 years and older were China, India, Japan, and Brazil ( United Nations, 2013 ). Because generalizable prevalence and incidence estimates are lacking in these countries, the exact load and burden of age-associated skin conditions can be estimated only.
Skin Aging and Economy
Worldwide older persons play important economic roles. On the one hand, they consume resources (e.g., income from savings, transfer from families or governments) and on the other hand, they spend money. How older people finance their consumption differs widely across countries. In many developing countries, they continue to work until very old ages, whereas in many developed countries, public transfers are the major source of old age support ( United Nations, 2013 ). However, in most countries, older people tend to give more than they receive to their family members (children, grandchildren; United Nations, 2013 ). Irrespective of which model applies, skin problems have a huge impact on working ability in the aged ( Morrone, 2008 ) and microeconomics. For instance, chronic wounds may lead to permanent disability leading to the inability to work. Wound management is also burdensome and costly leading to a heavy socioeconomic burden ( Sen et al., 2009 ). Skin aging and prevention of its negative effects have been inadequately addressed to the detriment of communities, societies, and economies around the world.
Defining Preventive Skin Care
Evidence-based interventions to maintain and to promote skin health during the life course are available. These involve and must require all parts of the health ecosystem—caregivers, general practitioners, nurses, hospital systems, and the aging individuals themselves—in the solutions. Recently, these preventive skin care approaches were formally defined and categorized into the primary, secondary, and tertiary prevention framework ( Kottner, Lichterfeld, Blume-Peytavi, & Kuhlmey, 2015 ; see Figure 3 ).
Figure 3.

Preventive skin care during the life course.
The goal of primary prevention is to protect healthy individuals from developing skin problems. UVR protection from birth until the end of life is the most important intervention, to avoid and/or to reduce UVR damage and skin cancer ( Cooley & Quale, 2013 ). Sun protective behavior includes the reduction of UVR exposure time, coverage of the head, face, and body, and by using sunscreens ( Carmel, Shani, & Rosenberg, 1996 ; Elsner et al., 2007 ; Ryan, 1998 ). However, the need for sun protection depends, among others, on the skin phototype and geographic region. Too strict sun protection may induce vitamin D deficiency. Therefore, a balance is needed between sun exposure needed for sufficient vitamin D levels and extrinsic skin aging and cancer prevention ( Jayaratne, Russell, & van der Pols, 2012 ; Ramankutty et al., 2014 ; Reichrath, 2006 ). Avoidance and/or the reduction of the exposure to irritants, allergens, or other molecules damaging the skin prevent and/or postpone the onset of contact or allergic dermatitis. This includes for instance the avoidance of harsh soaps, over-usage of skin care products ( Ananthapadmanabhan, Moore, Subramanyan, Misra, & Meyer, 2004 ), and skin protection, where necessary, at the workplace ( Ryan, 1998 ; Schwanitz et al., 2003 ).
Secondary prevention includes interventions for early diagnosis and treatment of existing (subclinical) skin problems. Self-examination and/or regular dermatologist visits to screen for early skin cancer helps to start treatment early thus improving patient outcome ( Federman, Kirsner, & Viola, 2013 ). Mild but manifested occupational skin diseases must be adequately treated to enable people affected to remain at their workplace ( Schwanitz et al., 2003 ). Secondary prevention also includes skin protection against lesions and wounds in the context of severe illness and in frail elderly patients like skin tears, superficial pressure ulcers, or incontinence-associated dermatitis ( Carville, Leslie, Osseiran-Moisson, Newall, & Lewin, 2014 ; Kottner, Lichterfeld, & Blume-Peytavi, 2013 ).
Tertiary prevention includes therapeutic and rehabilitative interventions once skin diseases are firmly established. For instance, individuals suffering from dry skin need targeted emollient therapy for symptom control and to maintain skin integrity ( Guenther et al., 2012 ). Pressure and venous ulcers need to be treated or at least controlled if wound healing is not the primary therapeutic goal.
Building a Public Health Approach on Skin Aging
Persisting Health Inequalities
Worldwide, there are huge inequalities regarding income, social status, health, and life expectancy ( Morrone, 2008 ; United Nations, 2013 ). These general disparities directly apply to skin health and age-associated skin conditions. Skin diseases and infestations are still very prevalent in developing countries ( Figueroa et al., 1998 ; Morrone, 2008 ; Perera, Atukorale, Sivayogan, Ariyaratne, & Karunaratne, 2000 ), whereas chronic inflammatory and oncologic skin diseases are more common in developed countries ( Finlay & Ryan, 1996 ). This pattern was recently confirmed by estimating the global mortality for skin diseases or diseases with skin manifestations based on latest Global Burden of Disease Study (2010; see Table 2 ; Boyers et al., 2014 ).
Differences Between Skin Disease–Related Mortality Between Developing and Developed Countries 2010 According to Boyers et al. (2014)
| Developed countries | Developing countries | |
|---|---|---|
| Melanoma | Higher | Lower |
| Basal and squamous cell carcinoma | Higher | Lower |
| Decubitus ulcer | Lower | Higher |
| Bacterial skin diseases | Lower | Higher |
| Cellulitis | Lower | Higher |
| Varicella | Lower | Higher |
| Syphilis | Lower | Higher |
| Measles | Lower | Higher |
| Dengue | No difference | |
| Other skin and subcutaneous diseases | Lower | Higher |
| Developed countries | Developing countries | |
|---|---|---|
| Melanoma | Higher | Lower |
| Basal and squamous cell carcinoma | Higher | Lower |
| Decubitus ulcer | Lower | Higher |
| Bacterial skin diseases | Lower | Higher |
| Cellulitis | Lower | Higher |
| Varicella | Lower | Higher |
| Syphilis | Lower | Higher |
| Measles | Lower | Higher |
| Dengue | No difference | |
| Other skin and subcutaneous diseases | Lower | Higher |
Differences Between Skin Disease–Related Mortality Between Developing and Developed Countries 2010 According to Boyers et al. (2014)
| Developed countries | Developing countries | |
|---|---|---|
| Melanoma | Higher | Lower |
| Basal and squamous cell carcinoma | Higher | Lower |
| Decubitus ulcer | Lower | Higher |
| Bacterial skin diseases | Lower | Higher |
| Cellulitis | Lower | Higher |
| Varicella | Lower | Higher |
| Syphilis | Lower | Higher |
| Measles | Lower | Higher |
| Dengue | No difference | |
| Other skin and subcutaneous diseases | Lower | Higher |
| Developed countries | Developing countries | |
|---|---|---|
| Melanoma | Higher | Lower |
| Basal and squamous cell carcinoma | Higher | Lower |
| Decubitus ulcer | Lower | Higher |
| Bacterial skin diseases | Lower | Higher |
| Cellulitis | Lower | Higher |
| Varicella | Lower | Higher |
| Syphilis | Lower | Higher |
| Measles | Lower | Higher |
| Dengue | No difference | |
| Other skin and subcutaneous diseases | Lower | Higher |
Table 2 indicates the death rates in developing countries were significantly higher for all skin conditions analyzed except melanoma, basal and squamous cell carcinoma, and dengue. In developing countries, more people die from infections such as cellulitis compared with developed countries indicating the inavailability of effective treatments or skills. It should be emphasized that most of these skin diseases require relatively low-technology health care strategies ( Ersser et al., 2011 ) and 90% of skin disease in tropical developing countries are diagnosed and treated by health care workers who have no dermatological training ( Morrone, 2008 ). Higher skin cancer mortality in the developed countries might be explained by the large proportion of fair-skinned population with their cultural emphasis on outdoor activities and indoor tanning services ( Boyers et al., 2014 ).
Improving Aging Skin Health Worldwide
The regional differences in skin disease risk and epidemiology require tailored management strategies, but at the core, information and access are the two most important key components for improving global skin health.
Developed Countries
Substantial variations in heath service provision within developed countries exist ( Morrone, 2008 ) but usually access to medical specialties like dermatology is possible. People with skin problems approach dermatologists directly or indirectly via referral. However, there are emerging discussions about a possible undersupply of dermatologists in some regions of Western societies to meet the increasing demand. In Europe, the density of dermatologists ranges from 1 per 100,000 of the population in the United Kingdom and to 1 per 20,000 in Italy and France ( Barker & Burgdorf, 2013 ). A density of 3.2 practicing dermatologists for every 100,000 people in the United States is considered too few ( Hilton, 2012 ).
Furthermore, the current efforts to reduce or control melanoma, and basal and squamous cell carcinoma in Western societies have failed during the past two decades ( Boyers et al., 2014 ). It is questionable whether more dermatological specialized care is able to tackle the ever-increasing skin cancer rates. Health care systems may benefit from integration of nursing expertise into primary care provision to promote skin healthier lifestyles or to enhance treatment compliance ( Ersser et al., 2011 ). Public health approaches are needed to promote sun protective behaviors including sun avoidance, wearing sun protective clothes, and use of sunscreens. Sunbeds must not be used at all. This might be achieved by intensified public awareness campaigns, education, or political actions to prevent sunbed use (e.g., like tobacco restriction; Kottner, Lichterfeld, et al., 2015 ). There is empirical evidence that health education programs can promote skin cancer protective behaviors even in the elderly ( Carmel et al., 1996 ).
Other age-associated conditions like dry skin, the increased risk for skin lesions, or wounds can be reduced by targeted skin care regimens. The use of low-irritant soaps and wash products and targeted leave-on skin care products containing emollients, humectants, and occlusives helps to improve skin barrier function and integrity and to reduce dryness and itch ( Cowdell & Steventon, 2015 ; Kottner et al., 2013 ). Depending on the care setting, primary caregivers like nurses are responsible for delivering appropriate skin care or care receivers and informal care givers need targeted education. Because of the close and continuous contact, nurses and other health care workers seem best placed to accomplish this task ( Ersser et al., 2011 ; Kottner, Boronat, et al., 2015 ).
Developing Countries
The major characteristic of developing country heath care is the absence of specialized care skills, particularly for skin diseases ( Ersser et al., 2011 ; Hay, Estrada, & Grossmann, 2011 ; Kaur, 2012 ). In addition, there are many regions where there are no, or few, trained health professionals and effective skin and wound management products are lacking ( Benskin, 2013 ). Because the majority of the world’s population lives in such resource-limited environments, there is an urgent need to take appropriate action and to eliminate such large health inequalities.
A major public health strategy to improve skin health worldwide is education to manage the common conditions and to identify skin signs of neglected tropical diseases ( Morrone, 2008 ). Numerous international initiatives have been launched successfully in developing and resource-poor regions using a community-based approach ( Figueroa et al., 1998 ; Hay et al., 2011 ). The main idea of community dermatology is to educate primary “frontline” caregivers to reach the maximum numbers of patients. These caregivers are clinical officers, village health workers, nurses, nurse assistants, or other trained staff ( Benskin, 2013 ). Empirical evidence suggests that even a single-day training may lead to a marked improvement in managing the most common skin diseases in these settings ( Mahé et al., 2005 ). In recent years, there has been a significant and growing contribution of nursing to improve skin care needs in the developing world including disabilities due to neglected diseases such as leprosy and filariasis ( Ersser et al., 2011 ; Kaur, 2012 ).
Despite the high load of infectious skin diseases in developing regions, other age-associated skin conditions are common in all areas. Dry skin and itch are the most common problems in the elderly and geriatric population in India, aggravated by incorrect use of soaps and cleansers ( Grover & Narasimhalu, 2009 ; Verma, 2011 ). Pigmentary changes, benign skin tumors, and dermatitis and eczema are most common in the aged in India and Sri Lanka ( Perera et al., 2000 ; Verma, 2011 ), which is comparable with developed countries.
Teleteaching and Teledermatology
The educational activities worldwide largely depend on local face-to-face teaching and training. However, web-based and mobile telephone–based applications are increasingly utilized to reach more health carers around the world ( Hay et al., 2011 ). Similarly, skin conditions can be detected and diagnosed by their appearance. Clinical or dermoscopic images can be shared immediately with experts. Skin care and dermatology may especially benefit from wider availability of communication technologies to improve patient outcomes ( Lotti, Handog, Hercogova, & Ramos-E-Silva, 2008 ).
Conclusions and Outlook
Prevention is far more effective and less costly than treatment ( World Health Organization, 2002 ). This is true for skin health ( Ryan, 1998 ) and it was recently emphasized during the 2014 Manchester Summit “A Life Course of Active Ageing and Healthy Skin: Identifying Challenges and Seizing Opportunities” ( Global Coalition on Aging, 2014 ). At this meeting, global aging and dermatology experts came together for an interdisciplinary and cross-geography dialogue about how to promote skin health. Based on the findings of this background paper and the summit discussion, the following key points can be identified so far:
-
Skin diseases become more prevalent as the aging population increases globally ( Global Coalition on Aging, 2014 ), which directly affects the functional capacity and overall health.
-
One in every three cancers diagnosed is skin cancer ( Global Coalition on Aging, 2014 ).
-
Many age-related dermatoses can best be managed by prevention ( Global Coalition on Aging, 2014 ; Gilchrest, 1986 ; Kottner, Lichterfeld, et al., 2015 ).
-
Effective strategies for protecting the skin are available, for example, UVR protection and protection against occupational hazards.
-
Skin hydration helps to treat and to prevent dry skin ( Global Coalition on Aging, 2014 ; Kottner et al., 2013 ; Kuo, Maslen, Keene, & Glanville, 1997 ).
-
In order to optimize skin health, skin protection must start as early as possible in life ( Elsner et al., 2007 ; Karonen, Jeskanen, & Keski-Oja, 1998 ); however, a balance should be found between overuse of topically applied products to avoid allergen exposure and underuse in people in need.
-
A wellness and prevention approach to protecting the skin from sun damage and other environmental factors can substantially reduce the incidence of nonmelanoma and other skin cancers ( Global Coalition on Aging, 2014 ).
-
Nursing and other health care professionals are directly relevant to preventing or managing skin diseases and associated physical, psychological, and social consequences in developing as well as in developed countries ( Ersser et al., 2011 ).
-
Older people are interested in and willing to participate in health promotion activities ( Miller & Iris, 2002 ). Means of adopting this knowledge on skin health promotion are poorly developed.
-
Healthy skin can lead to better mental and emotional health with positive impact on social engagement ( Global Coalition on Aging, 2014 ).
-
As older people are frequently excluded from clinical trials, research is needed to guide practice decisions regarding common skin problems and wounds in the elderly ( Chang et al., 2013 ; Karonen et al., 1998 ).
-
Maintaining a healthier skin when we are older enables greater health and is the basis for more active and engaged lives.
Combined, the impact of aging skin on the overall health ecosystem will be exponential compared with decades past because of 21st century aging. These pressures on the public health system, however, can be alleviated by a more effective preventive approach to skin health as we age.
References
Adam
J. E.
, &
Reilly
S
. (
1987
).
The prevalence of skin disease in the geriatric age group
.
The Australasian Journal of Dermatology
,
28
,
72
–
76
.
Al-Nuaimi
Y.
Sherratt
M. J.
, &
Griffiths
C. E
. (
2014
).
Skin health in older age
.
Maturitas
,
79
,
256
–
264
. doi:
Ananthapadmanabhan
K. P.
Moore
D. J.
Subramanyan
K.
Misra
M.
, &
Meyer
F
. (
2004
).
Cleansing without compromise: The impact of cleansers on the skin barrier and the technology of mild cleansing
.
Dermatologic Therapy
,
17
(
Suppl. 1
),
16
–
25
.
Aronson
L
. (
2015
).
The human lifecycle’s neglected stepchild
.
Lancet (London, England)
,
385
,
500
–
501
.
Autio
P.
Risteli
J.
Haukipuro
K.
Risteli
L.
, &
Oikarinen
A
. (
1994
).
Collagen synthesis in human skin in vivo: Modulation by aging, ultraviolet B irradiation and localization
.
Photodermatology, Photoimmunology & Photomedicine
,
10
,
212
–
216
.
Bailey
A. J
. (
2001
).
Molecular mechanisms of ageing in connective tissues
.
Mechanisms of Ageing and Development
,
122
,
735
–
755
. doi:10.1016/S0047-6374(01)00225-1
Barker
J.
,
&
Burgdorf
. (
2013
).
The challenge of skin diseases in Europe
(
4
th ed.).
Berlin
:
ABW Wissenschaftsverlag
.
Beauregard
S.
, &
Gilchrest
B. A
. (
1987
).
A survey of skin problems and skin care regimens in the elderly
.
Archives of Dermatology
,
123
,
1638
–
1643
. doi:10.1001/archderm.1987.01660360066014
Beier
W
. (
1985
).
[The concept of vitality and the Ries biological index]
.
Zeitschrift für Gerontologie
,
18
,
353
–
357
.
Benskin
L. L
. (
2013
).
A review of the literature informing affordable, available wound management choices for rural areas of tropical developing countries
.
Ostomy/Wound Management
,
59
,
20
–
41
.
Berger
T. G.
Shive
M.
, &
Harper
G. M
. (
2013
).
Pruritus in the older patient: A clinical review
.
Journal of American Medical Assoiation
,
310
,
2443
–
2450
. doi:
Bilgili
S. G.
Karadag
A. S.
Ozkol
H. U.
Calka
O.
, &
Akdeniz
N
. (
2012
).
The prevalence of skin diseases among the geriatric patients in Eastern Turkey
.
Journal of Pakistan Medical Association
,
62
,
535
–
539
.
Bilgili
M. E.
Yildiz
H.
, &
Sarici
G
. (
2013
).
Prevalence of skin diseases in a dermatology outpatient clinic in Turkey. A cross-sectional, retrospective study
.
Journal of Dermatological Case Reports
,
7
,
108
–
112
. doi:
Bolognia
J. L.
Braverman
I. M.
Rousseau
M. E.
, &
Sarrel
P. M
. (
1989
).
Skin changes in menopause
.
Maturitas
,
11
,
295
–
304
.
Boyers
L. N.
Karimkhani
C.
Naghavi
M.
Sherwood
D.
Margolis
D. J.
Hay
R. J.
, …
Dellavalle
R. P
. (
2014
).
Global mortality from conditions with skin manifestations
.
Journal of the American Academy of Dermatology
,
71
,
1137
–
1143.e17
. doi:
Braverman
I. M.
, &
Fonferko
E
. (
1982
).
Studies in cutaneous aging .1. The elastic fiber network
.
Journal of Investigative Dermatology
,
78
,
434
–
443
. doi:
Brincat
M.
Moniz
C. F.
Studd
J. W.
Darby
A. J.
Magos
A.
, &
Cooper
D
. (
1983
).
Sex hormones and skin collagen content in postmenopausal women
.
British Medical Journal (Clinical Research Ed.)
,
287
,
1337
–
1338
.
Carmel
S.
Shani
E.
, &
Rosenberg
L
. (
1996
).
Skin cancer protective behaviors among the elderly: Explaining their response to a health education program using the health belief model
.
Educational Gerontology
,
22
,
651
–
668
. doi:
Carville
K.
Leslie
G.
Osseiran-Moisson
R.
Newall
N.
, &
Lewin
G
. (
2014
).
The effectiveness of a twice-daily skin-moisturising regimen for reducing the incidence of skin tears
.
International Wound Journal
,
11
,
446
–
453
. doi:
Chang
A. L.
Wong
J. W.
Endo
J. O.
, &
Norman
R. A
. (
2013
).
Geriatric dermatology review: Major changes in skin function in older patients and their contribution to common clinical challenges
.
Journal of the American Medical Directors Association
,
14
,
724
–
730
. doi:
Choi
E. H.
Man
M. Q.
Xu
P.
Xin
S.
Liu
Z.
Crumrine
D. A.
, …
Mauro
T. M
. (
2007
).
Stratum corneum acidification is impaired in moderately aged human and murine skin
.
The Journal of Investigative Dermatology
,
127
,
2847
–
2856
. doi:
Chuong
C. M.
Nickoloff
B. J.
Elias
P. M.
Goldsmith
L. A.
Macher
E.
Maderson
P. A.
, …
Christophers
E
. (
2002
).
What is the ‘true’ function of skin?
Experimental Dermatology
,
11
,
159
–
187
. doi:10.1034/j.1600-0625.2002.00112.x
Cooley
J. H.
, &
Quale
L. M
. (
2013
).
Skin cancer preventive behavior and sun protection recommendations
.
Seminars in Oncology Nursing
,
29
,
223
–
226
. doi:
Cowdell
F
. (
2011
).
Older people, personal hygiene, and skin care
.
Medsurg Nursing
,
20
,
235
–
240
.
Cowdell
F.
, &
Steventon
K
. (
2015
).
Skin cleansing practices for older people: A systematic review
.
International Journal of Older People Nursing
,
10
,
3
–
13
. doi:
Daly
C. H
. (
1982
).
Biomechanical properties of dermis
.
The Journal of Investigative Dermatology
,
79
(
Suppl. 1
),
17s
–
20s
.
Daniell
H. W
. (
1971
).
Smoker’s wrinkles. A study in the epidemiology of “crow’s feet”
.
Annals of Internal Medicine
,
75
,
873
–
880
. doi:10.7326/0003-4819-75-6-873
Darjani
A.
Mohtasham-Amiri
Z.
Mohammad Amini
K.
Golchai
J.
Sadre-Eshkevari
S.
, &
Alizade
N
. (
2013
).
Skin disorders among elder patients in a Referral Center in Northern Iran (2011)
.
Dermatology Research and Practice
,
2013
,
193205
. doi:
Dawber
R.
, &
Shuster
S
. (
1971
).
Scanning electron microscopy of dermal fibrous tissue networks in normal skin, solar elastosis and pseudo-xanthoma elasticum
.
British Journal of Dermatology
,
84
,
130
–
134
. doi:
Dobos
G.
Lichterfeld
A.
Blume-Peytavi
U.
, &
Kottner
J
. (
2015
).
Evaluation of skin ageing: A systematic review of clinical scales
.
British Journal of Dermatology
,
172
,
1249
–
1261
. doi:
Elsner
P.
Holzle
E.
Diepgen
T.
Grether-Beck
S.
Honigsmann
H.
Krutmann
J.
, …
Luger
T
. (
2007
).
Recommendation: Daily sun protection in the prevention of chronic UV-induced skin damage
.
Journal der Deutschen dermatologischen Gesellschaft
,
5
,
166
–
173
. doi:
Emmerson
E.
, &
Hardman
M. J
. (
2012
).
The role of estrogen deficiency in skin ageing and wound healing
.
Biogerontology
,
13
,
3
–
20
. doi:
Ersser
S. J.
Kaur
V.
Kelly
P.
Langøen
A.
Maguire
S. A.
Nicol
N. H.
, …
Ward
C
. (
2011
).
The contribution of the nursing service worldwide and its capacity to benefit within the dermatology field
.
International Journal of Dermatology
,
50
,
582
–
589
. doi:
Farage
M. A.
Miller
K. W.
Berardesca
E.
, &
Maibach
H. I
. (
2010
).
Psychological and social implications of aging skin: Normal aging and the effects of cutaneous disease
. In
M. A.
Farage
K. W.
Miller
, &
H. I.
Maibach
(Eds.),
Textbook of ageing skin
(pp.
949
–
959
).
Berlin
:
Springer
.
Federman
D. G.
Kirsner
R. S.
, &
Viola
K. V
. (
2013
).
Skin cancer screening and primary prevention: Facts and controversies
.
Clinics in Dermatology
,
31
,
666
–
670
. doi:
Figueroa
J. I.
Fuller
L. C.
Abraha
A.
, &
Hay
R. J
. (
1998
).
Dermatology in southwestern Ethiopia: Rationale for a community approach
.
International Journal of Dermatology
,
37
,
752
–
758
. doi:10.1046/j.1365-4362.1998.00425.x
Finlay
A. Y.
, &
Ryan
T. J
. (
1996
).
Disability and handicap in dermatology
.
International Journal of Dermatology
,
35
,
305
–
311
. doi:10.1111/j.1365-4362.1996.tb03628.x
Fleischer
A. B.
McFarlane
M.
Hinds
M. A.
, &
Mittelmark
M. B
. (
1996
).
Skin conditions and symptoms are common in the elderly: The prevalence of skin symptoms and conditions in an elderly population
.
Journal of Geriatric Dermatology
,
4
,
78
–
87
.
Fuchs
E
. (
2009
).
Finding one’s niche in the skin
.
Cell Stem Cell
,
4
,
499
–
502
. doi:
Furth
J. J
. (
1991
).
The steady-state levels of type I collagen mRNA are reduced in senescent fibroblasts
.
Journal of Gerontology
,
46
,
B122
–
B124
. doi:10.1093/geronj/46.3.B122
Garibyan
L.
Chiou
A. S.
, &
Elmariah
S. B
. (
2013
).
Advanced aging skin and itch: Addressing an unmet need
.
Dermatologic Therapy
,
26
,
92
–
103
. doi:
Giangreco
A.
Goldie
S. J.
Failla
V.
Saintigny
G.
, &
Watt
F. M
. (
2010
).
Human skin aging is associated with reduced expression of the stem cell markers beta1 integrin and MCSP
.
The Journal of Investigative Dermatology
,
130
,
604
–
608
. doi:
Gilchrest
B. A
. (
1986
).
Geriatric skin problems
.
Hospital Practice (Off Ed)
,
21
,
55, 59
–
65
.
Gorecki
C.
Brown
J. M.
Nelson
E. A.
Briggs
M.
Schoonhoven
L.
Dealey
C.
,
…
European Quality of Life Pressure Ulcer Project Group
. (
2009
).
Impact of pressure ulcers on quality of life in older patients: A systematic review
.
Journal of the American Geriatrics Society
,
57
,
1175
–
1183
. doi:
Gould
L.
Abadir
P.
Brem
H.
Carter
M.
Conner-Kerr
T.
Davidson
J.
, …
Schmader
K
. (
2015
).
Chronic wound repair and healing in older adults: Current status and future research
.
Wound Repair and Regeneration
,
63
,
427
–
438
. doi:
Graham
H. K.
Hodson
N. W.
Hoyland
J. A.
Millward-Sadler
S. J.
Garrod
D.
Scothern
A.
, …
Sherratt
M. J
. (
2010
).
Tissue section AFM: In situ ultrastructural imaging of native biomolecules
.
Matrix Biology
,
29
,
254
–
260
. doi:
Grover
S.
, &
Narasimhalu
C. R
. (
2009
).
A clinical study of skin changes in geriatric population
.
Indian Journal of Dermatology, Venereology and Leprology
,
75
,
305
–
306
. doi:
Guenther
L.
Lynde
C. W.
Andriessen
A.
Barankin
B.
Goldstein
E.
Skotnicki
S. P.
, …
Sloan
K
. (
2012
).
Pathway to dry skin prevention and treatment
.
Journal of Cutaneous Medicine and Surgery
,
16
,
23
–
31
.
Gupta
M. A
. (
2010
).
Aging skin: Some psychosomatoc aspects
. In
M. A.
Farage
K. W.
Miller
, &
H. I.
Maibach
(Eds.),
Textbook of ageing skin
(pp.
959
–
969
).
Berlin
:
Springer
.
Gupta
M. A.
, &
Gilchrest
B. A
. (
2005
).
Psychosocial aspects of aging skin
.
Dermatologic Clinics
,
23
,
643
–
648
. doi:
Hatje
L. K.
Richter
C.
Blume-Peytavi
U.
, &
Kottner
J
. (
2015
).
Blistering time as a parameter for the strength of dermoepidermal adhesion: A systematic review and meta-analysis
.
The British Journal of Dermatology
,
172
,
323
–
330
. doi:
Hay
R.
Estrada
R.
, &
Grossmann
H
. (
2011
).
Managing skin disease in resource-poor environments – the role of community-oriented training and control programs
.
International Journal of Dermatology
,
50
,
558
–
563
. doi:
Hay
R. J.
Johns
N. E.
Williams
H. C.
Bolliger
I. W.
Dellavalle
R. P.
Margolis
D. J.
, …
Naghavi
M
. (
2014
).
The global burden of skin disease in 2010: An analysis of the prevalence and impact of skin conditions
.
The Journal of Investigative Dermatology
,
134
,
1527
–
1534
. doi:
Hull
M. T.
, &
Warfel
K. A
. (
1983
).
Age-related changes in the cutaneous basal lamina: Scanning electron microscopic study
.
The Journal of Investigative Dermatology
,
81
,
378
–
380
. doi:10.1111/1523-1747.ep12519989
Jayaratne
N.
Russell
A.
, &
van der Pols
J. C
. (
2012
).
Sun protection and vitamin D status in an Australian subtropical community
.
Preventive Medicine
,
55
,
146
–
150
. doi:
Jensen
J. M.
Förl
M.
Winoto-Morbach
S.
Seite
S.
Schunck
M.
Proksch
E.
, &
Schütze
S
. (
2005
).
Acid and neutral sphingomyelinase, ceramide synthase, and acid ceramidase activities in cutaneous aging
.
Experimental Dermatology
,
14
,
609
–
618
. doi:
Jurciukonyte
R.
Vincerzevskiene
I.
Krilaviciute
A.
Bylaite
M.
, &
Smailyte
G
. (
2013
).
Epidemiology of basal cell carcinoma in Lithuania, 1996-2010
.
The British Journal of Dermatology
,
169
,
1100
–
1105
. doi:
Kadoya
K.
Sasaki
T.
Kostka
G.
Timpl
R.
Matsuzaki
K.
Kumagai
N.
, …
Amano
S
. (
2005
).
Fibulin-5 deposition in human skin: Decrease with ageing and ultraviolet B exposure and increase in solar elastosis
.
The British Journal of Dermatology
,
153
,
607
–
612
. doi:
Kadunce
D. P.
Burr
R.
Gress
R.
Kanner
R.
Lyon
J. L.
, &
Zone
J. J
. (
1991
).
Cigarette smoking: Risk factor for premature facial wrinkling
.
Annals of Internal Medicine
,
114
,
840
–
844
. doi:10.7326/0003-4819-114-10-840
Karamichos
D.
Lakshman
N.
, &
Petroll
W. M
. (
2007
).
Regulation of corneal fibroblast morphology and collagen reorganization by extracellular matrix mechanical properties
.
Investigative Ophthalmology & Visual Science
,
48
,
5030
–
5037
. doi:
Karonen
T.
Jeskanen
L.
, &
Keski-Oja
J
. (
1998
).
Transforming growth factor-beta 1 and its latent form binding protein-1 associate with elastic fibres in human dermis
.
Molecular Biology of the Cell
,
9
,
304a
–
304a
. doi:10.1046/j.1365-2133.1997.17671859.x
Kaur
V
. (
2012
).
Dermatology nursing in India: The journey thus far
.
Indian Journal of Dermatology, Venereology and Leprology
,
78
,
527
–
531
. doi:
Kaya
G.
, &
Saurat
J. H
. (
2007
).
Dermatoporosis: A chronic cutaneous insufficiency/fragility syndrome. Clinicopathological features, mechanisms, prevention and potential treatments
.
Dermatology (Basel, Switzerland)
,
215
,
284
–
294
. doi:
Kaya
G.
Tran
C.
Sorg
O.
Hotz
R.
Grand
D.
Carraux
P.
, …
Saurat
J. H
. (
2006
).
Hyaluronate fragments reverse skin atrophy by a CD44-dependent mechanism
.
PLoS Medicine
,
3
,
e493
. doi:
Kiliç
A.
Gül
U.
Aslan
E.
, &
Soylu
S
. (
2008
).
Dermatological findings in the senior population of nursing homes in Turkey
.
Archives of Gerontology and Geriatrics
,
47
,
93
–
98
. doi:
Kottner
J.
Boronat
X.
Blume-Peytavi
U.
Lahmann
N.
, &
Suhr
R
. (
2015
).
The epidemiology of skin care provided by nurses at home: A multicentre prevalence study
.
Journal of Advanced Nursing
,
71
,
570
–
580
. doi:
Kottner
J.
Lichterfeld
A.
, &
Blume-Peytavi
U
. (
2013
).
Maintaining skin integrity in the aged: A systematic review
.
The British Journal of Dermatology
,
169
,
528
–
542
. doi:
Kottner
J.
Lichterfeld
A.
Blume-Peytavi
U.
, &
Kuhlmey
A
. (
2015
).
Skin health promotion in the elderly
.
Zeitschrift für Gerontologie und Geriatrie
, 48, 231–236. doi:
Krutmann
J.
Liu
W.
Li
L.
Pan
X.
Crawford
M.
Sore
G.
, &
Seite
S
. (
2014
).
Pollution and skin: From epidemiological and mechanistic studies to clinical implications
.
Journal of Dermatological Science
,
76
,
163
–
168
. doi:
Kuh
D.
Richards
M.
Cooper
R.
Hardy
R.
, &
Ben-Shlomo
Y
. (
2014
).
Life course epidemiology, ageing research, and maturing cohort studies: A dynamic combination for understanding healthy ageing
. In
D.
Kuh
R.
Cooper
R.
Hardy
M.
Richards
, &
Y.
Ben-Shlomo
(Eds.),
A life course approach to healthy ageing
(pp.
3
–
15
).
Oxford
:
Oxford University Press
.
Kuo
H. J.
Maslen
C. L.
Keene
D. R.
, &
Glanville
R. W
. (
1997
).
Type VI collagen anchors endothelial basement membranes by interacting with type IV collagen
.
The Journal of Biological Chemistry
,
272
,
26522
–
26529
. doi:10.1074/jbc.272.42.26522
Lane
C. G.
, &
Rockwood
E. M
. (
1949
).
Geriatric dermatoses
.
The New England Journal of Medicine
,
241
,
772
–
777
. doi:
Lavker
R. M.
Zheng
P. S.
, &
Dong
G
. (
1987
).
Aged skin: A study by light, transmission electron, and scanning electron microscopy
.
The Journal of Investigative Dermatology
,
88
(
3 Suppl
.),
44s
–
51s
.
Liao
Y. H.
Chen
K. H.
Tseng
M. P.
, &
Sun
C. C
. (
2001
).
Pattern of skin diseases in a geriatric patient group in Taiwan: A 7-year survey from the outpatient clinic of a university medical center
.
Dermatology (Basel, Switzerland)
,
203
,
308
–
313
. doi:10.1159/000051778
Lotti
T.
Handog
E. B.
Hercogova
J.
, &
Ramos-E-Silva
M
. (
2008
).
International dermatology: The many faces and challenges of the specialty in the global village
.
Dermatologic Clinics
,
26
,
183
–
90, v
. doi:
Lovell
C. R.
Smolenski
K. A.
Duance
V. C.
Light
N. D.
Young
S.
, &
Dyson
M
. (
1987
).
Type I and III collagen content and fibre distribution in normal human skin during ageing
.
The British Journal of Dermatology
,
117
,
419
–
428
. doi:10.1111/j.1365-2133.1987.tb04921.x
Mahé
A.
Faye
O.
N’Diaye
H. T.
Konaré
H. D.
Coulibaly
I.
Kéita
S.
, …
Hay
R. J
. (
2005
).
Integration of basic dermatological care into primary health care services in Mali
.
Bulletin of the World Health Organization
,
83
,
935
–
941
. doi:
Martires
K. J.
Fu
P.
Polster
A. M.
Cooper
K. D.
, &
Baron
E. D
. (
2009
).
Factors that affect skin aging: A cohort-based survey on twins
.
Archives of Dermatology
,
145
,
1375
–
1379
. doi:
Mayer
J. E.
Swetter
S. M.
Fu
T.
, &
Geller
A. C
. (
2014
).
Screening, early detection, education, and trends for melanoma: Current status (2007-2013) and future directions: Part II. Screening, education, and future directions
.
Journal of the American Academy of Dermatology
,
71
,
611.e1
–
611.e10
; quiz 621. doi:
Miller
A. M.
, &
Iris
M
. (
2002
).
Health promotion attitudes and strategies in older adults
.
Health Education & Behaviour
,
29
,
249
–
267
. doi:10.1177/109019810202900209
Morrone
A
. (
2008
).
Poverty, dignity, and forgotten skin care: Dermatology in the stream of human mobile population
.
Dermatologic Clinics
,
26
,
245
–
256, vi
. doi:
Pearce
R. H.
, &
Grimmer
B. J
. (
1972
).
Age and the chemical constitution of normal human dermis
.
The Journal of Investigative Dermatology
,
58
,
347
–
361
. doi:10.1111/1523-1747.ep12540531
Perera
A.
Atukorale
D. N.
Sivayogan
S.
Ariyaratne
V. S.
, &
Karunaratne
L. A
. (
2000
).
Prevalence of skin diseases in suburban Sri Lanka
.
The Ceylon Medical Journal
,
45
,
123
–
128
.
Ramankutty
P.
de Klerk
N. H.
Miller
M.
Fenech
M.
O’Callaghan
N.
Armstrong
B. K.
, &
Milne
E
. (
2014
).
Ultraviolet radiation exposure and serum vitamin D levels in young children
.
Journal of Paediatrics and Child Health
,
50
,
713
–
720
. doi:
Reed
R. K.
Lilja
K.
, &
Laurent
T. C
. (
1988
).
Hyaluronan in the rat with special reference to the skin
.
Acta Physiologica Scandinavica
,
134
,
405
–
411
. doi:
Reichrath
J
. (
2006
).
The challenge resulting from positive and negative effects of sunlight: How much solar UV exposure is appropriate to balance between risks of vitamin D deficiency and skin cancer?
Progress in Biophysics and Molecular Biology
,
92
,
9
–
16
. doi:
Ritz-Timme
S.
Laumeier
I.
, &
Collins
M. J
. (
2003
).
Aspartic acid racemization: Evidence for marked longevity of elastin in human skin
.
The British Journal of Dermatology
,
149
,
951
–
959
. doi:10.1111/j.1365-2133.2003.05618.x
Ruiz-Torres
A.
Agudo
A.
Vicent
D.
, &
Beier
W
. (
1990
).
Measuring human aging using a two-compartmental mathematical model and the vitality concept
.
Archives of Gerontology and Geriatrics
,
10
,
69
–
76
. doi:10.1016/0167-4943(90)90045-8
Ryan
T. J
. (
1992
).
Worldwide strategy for skin health care in a financial strait-jacket
.
International Journal of Dermatology
,
31
,
416
–
421
. doi:10.1111/j.1365-4362.1992.tb02672.x
Ryan
T. J
. (
1998
).
Healthy skin for all in a threatening environment
.
Clinics in Dermatology
,
16
,
181
–
184
. doi:10.1016/S0738-081X(97)00195-8
Schwanitz
H. J.
Riehl
U.
Schlesinger
T.
Bock
M.
Skudlik
C.
, &
Wulfhorst
B
. (
2003
).
Skin care management: Educational aspects
.
International Archives of Occupational and Environmental Health
,
76
,
374
–
381
. doi:
Sen
C. K.
Gordillo
G. M.
Roy
S.
Kirsner
R.
Lambert
L.
Hunt
T. K.
, …
Longaker
M. T
. (
2009
).
Human skin wounds: A major and snowballing threat to public health and the economy
.
Wound Repair and Regeneration
,
17
,
763
–
771
. doi:
Shapiro
S. D.
Endicott
S. K.
Province
M. A.
Pierce
J. A.
, &
Campbell
E. J
. (
1991
).
Marked longevity of human lung parenchymal elastic fibers deduced from prevalence of D-aspartate and nuclear weapons-related radiocarbon
.
The Journal of Clinical Investigation
,
87
,
1828
–
1834
. doi:
Sherwin
M. A.
, &
Gastwirth
C. M
. (
1990
).
Detrimental effects of cigarette smoking on lower extremity wound healing
.
The Journal of Foot Surgery
,
29
,
84
–
87
.
Siragusa
M.
Schepis
C.
Palazzo
R.
Fabrizi
G.
Guarneri
B.
Del Gracco
S.
, …
Ferri
R
. (
1999
).
Skin pathology findings in a cohort of 1500 adult and elderly subjects
.
International Journal of Dermatology
,
38
,
361
–
366
. doi:10.1046/j.1365-4362.1999.00720.x
Smith
D. R.
Sheu
H. M.
Hsieh
F. S.
Lee
Y. L.
Chang
S. J.
, &
Guo
Y. L
. (
2002
).
Prevalence of skin disease among nursing home patients in southern Taiwan
.
International Journal of Dermatology
,
41
,
754
–
759
. doi:10.1046/j.1365-4362.2002.01425.x
Sørensen
L. T.
Toft
B. G.
Rygaard
J.
Ladelund
S.
Paddon
M.
James
T.
, …
Gottrup
F
. (
2010
).
Effect of smoking, smoking cessation, and nicotine patch on wound dimension, vitamin C, and systemic markers of collagen metabolism
.
Surgery
,
148
,
982
–
990
. doi:
Tindall
J. P
. (
1976
).
Skin changes and lesions in our senior citizens: Incidences
.
Cutis
,
18
,
359
–
362
.
Tindall
J. P.
, &
Smith
J. G.
Jr
. (
1963
).
Skin lesions of the aged and their association with internal changes
.
Journal of American Medical Assoiation
,
186
,
1039
–
1042
. doi:10.1001/jama.1963.03710120021004
United Nations, Department of Economic and Social Affairs, Population Division. (2013). World Population Ageing 2013. ST/ESA/SER.A/348
.
Verma
S. B
. (
2011
).
Dermatology for the elderly: An Indian perspective
.
Clinics in Dermatology
,
29
,
91
–
96
. doi:
Warren
R.
Gartstein
V.
Kligman
A. M.
Montagna
W.
Allendorf
R. A.
, &
Ridder
G. M
. (
1991
).
Age, sunlight, and facial skin: A histologic and quantitative study
.
Journal of the American Academy of Dermatology
,
25
(
5 Pt. 1
),
751
–
760
. doi:10.1016/S0190-9622(08)80964-4
Weismann
K.
Krakauer
R.
, &
Wanscher
B
. (
1980
).
Prevalence of skin diseases in old age
.
Acta Dermato-venereologica
,
60
,
352
–
353
.
White-Chu
E. F.
, &
Reddy
M
. (
2011
).
Dry skin in the elderly: Complexities of a common problem
.
Clinics in Dermatology
,
29
,
37
–
42
. doi:
Whittaker
P.
, &
Canham
P. B
. (
1991
).
Demonstration of quantitative fabric analysis of tendon collagen using two-dimensional polarized light microscopy
.
Matrix (Stuttgart, Germany)
,
11
,
56
–
62
.
Yalçin
B.
Tamer
E.
Toy
G. G.
Oztaş
P.
Hayran
M.
, &
Alli
N
. (
2006
).
The prevalence of skin diseases in the elderly: Analysis of 4099 geriatric patients
.
International Journal of Dermatology
,
45
,
672
–
676
. doi:
Yap
K. B.
Siew
M. G.
, &
Goh
C. L
. (
1994
).
Pattern of skin diseases in the elderly seen at the National Skin Centre (Singapore) 1990
.
Singapore Medical Journal
,
35
,
147
–
150
.
Author notes
© The Author 2016. Published by Oxford University Press on behalf of The Gerontological Society of America. All rights reserved. For permissions, please e-mail: [email protected].
© The Author 2016. Published by Oxford University Press on behalf of The Gerontological Society of America. All rights reserved. For permissions, please e-mail: [email protected].
[ad_2]
Source link